The "kiss of life" is the everyday name for expired air resuscitation (EAR), also called mouth-to-mouth resuscitation. A rescuer breathes their own exhaled air into a victim who has stopped breathing. That breath still carries about 16-17% oxygen, enough to keep vital organs supplied until normal breathing returns or help arrives.
The “kiss of life” is really expired air resuscitation, and the air you breathe out still carries enough oxygen to keep someone alive.
Being able to give a person a fresh lease on life is undoubtedly one of the rarest and purest gifts that one can give. This can come in various forms, both practically and theoretically.
I’m sure that all of us have seen, at some point, either in movies, books, or personal experience, that when someone is dying as a result of drowning, anaphylactic shock, asthma attack, or the likes, they are often given the “kiss of life”.
Expired Air Resuscitation
In movies, a person is often seen passed out from drowning or gasping for breath. They then have a savior enter the scene dramatically, and breathe into the victim’s mouth, until the rising and falling of the victim’s chest resumes its normal rhythm. Colloquially called the kiss of life, the technical term is expired air resuscitation (EAR).
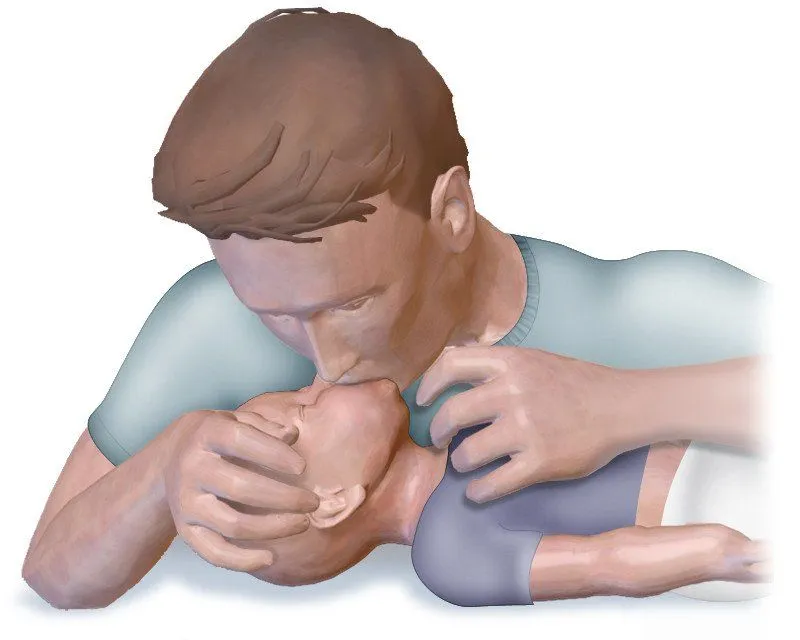
This is a form of artificial breathing or ventilation wherein the victim requires assistance in normal breathing. Air is forced down their respiratory tract until it reaches the lungs. This is done a number of times until that person can breathe on their own or until medical help arrives.
EAR is different from CPR, although the two are often used together for better results.
How Does It Work?
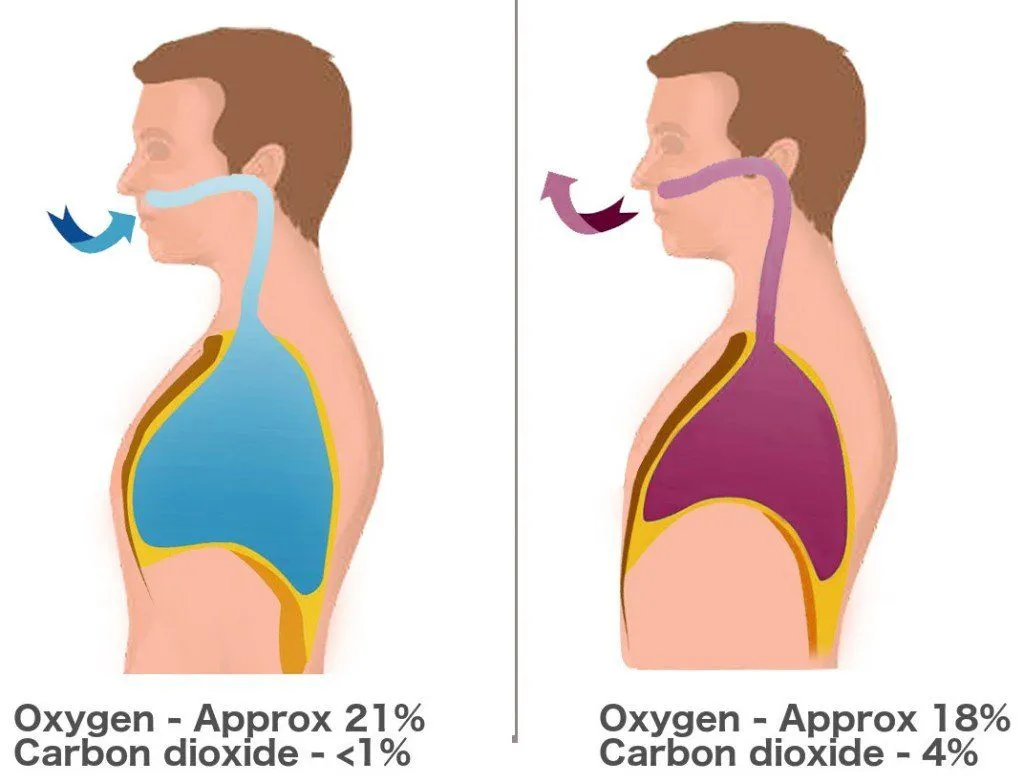
When performing EAR on a person, we force our exhaled air into their mouth. However, basic biology tells us that the air we exhale is low in oxygen, and higher in carbon dioxide. Therefore, it is normal to wonder about the effectiveness of EAR. If a person is already in distress, then blowing carbon dioxide into them should bring about a negative effect, right?
The answer lies in understanding the composition of the air that we inhale and expire. The former has approximately 21% oxygen and less than 1% carbon dioxide. Once the air enters our lungs, gaseous exchange takes place. The air that we exhale contains about 4-5% carbon dioxide and 16-17% oxygen. That’s correct! On a single breath, our body absorbs only about a quarter of the oxygen we take in, so most of it comes straight back out.
A person who requires EAR is usually in danger of dying from hypoxia, or loss of oxygen. In such a case, it is imperative that they receive oxygen. Therefore, although the oxygen content is less in our expired air, it can still work to revive a person. After all, half a loaf is better than no bread at all!
Precautions To Be Taken
EAR can be effective, provided that it is performed correctly. First and foremost, it is essential to be able to differentiate when EAR should be performed. The basic purpose of EAR is to resume a person’s normal breathing. However, if the heart isn’t beating, rescue breaths alone won't help. Modern first aid guidance no longer asks an untrained rescuer to hunt for a pulse, because a faint pulse is easy to miss and the delay can cost precious seconds. Instead, if a person is unresponsive and not breathing normally, you should start CPR right away (chest compressions, with rescue breaths if you are trained and willing) and call for emergency help.
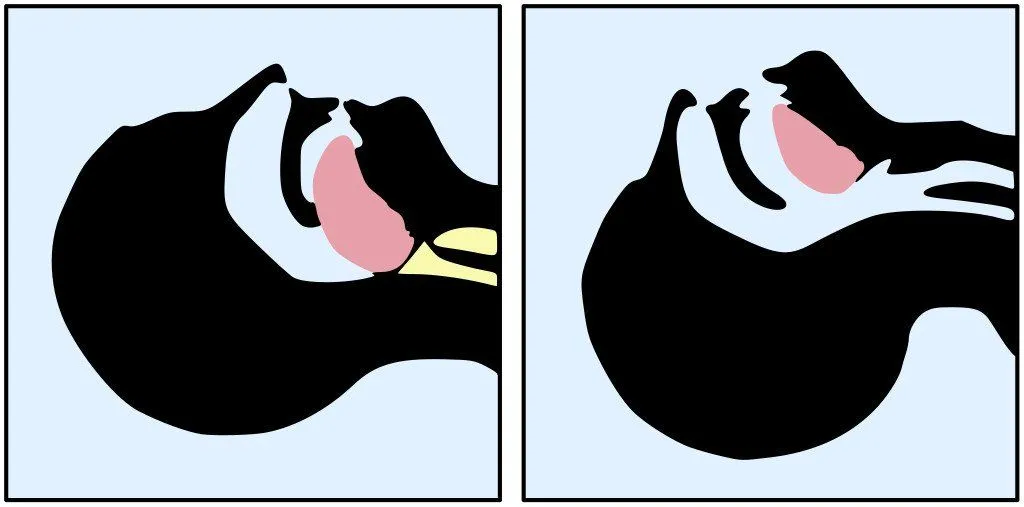
Artificial ventilation will only be effective if there is no obstruction in the airway. If something is blocking the windpipe, like the tongue or any other object, it should first be removed or moved out of the way. Another thing that must be kept in mind is that the air must enter the correct pipe. When performing EAR, care should be taken to observe which part of the victim’s body is rising and falling. If it is the stomach, it means that the air is entering the wrong pipe, and the angle of breathing should be changed.
While blowing into a person’s mouth, one should be careful not to over-inflate the victim’s lungs. This can be gauged by the rising of the chest. The moment the victim’s chest begins to rise, the air should be allowed to escape the lungs before the next effective breath is delivered to the person.
Resuscitation of a person usually requires medical aid, aside from these first aid techniques. Therefore, it is always advisable to get checked by a registered physician, even if the victim claims to feel completely fine. It should also be kept in mind that these techniques must be performed with caution, as there are a number of other factors that could affect the person, such as injuries, tears, etc. Therefore, it is best if a trained person is entrusted with this potentially life-saving task.
What Does EAR Stand For, And Where Does It Fit Into First Aid?
If you have ever stumbled over the acronym in a first aid quiz, here is the plain answer: EAR stands for Expired Air Resuscitation. "Expired air" simply means the air you breathe out, and "resuscitation" means reviving someone. Put together, it describes exactly what the kiss of life does, namely using the rescuer's own exhaled breath to ventilate a victim who has stopped breathing. The very same action is what first aiders call a rescue breath, so "expired air resuscitation", "rescue breathing", and "mouth-to-mouth" all point to the one technique.

So where does a rescue breath actually fit into the bigger picture? Modern first aid teaches a single ordered checklist, often remembered by the letters DRSABCD: check for Danger, check for Response, Send for help, open the Airway, check Breathing, start CPR, and use a Defibrillator if one is available. Rescue breaths sit inside that "B" and "C" stage. If the person is unresponsive and not breathing normally, you begin CPR, which pairs chest compressions with rescue breaths.
For an adult, the standard pattern is 30 chest compressions followed by 2 rescue breaths (written as 30:2), repeated until help arrives, with compressions delivered at a rate of about 100 to 120 per minute. To give the breath itself, you tilt the head back, lift the chin to open the airway, pinch the soft part of the nose shut, seal your lips over the person's mouth, and blow steadily for about one second while watching the chest rise. One honest caveat from current guidance: if you are untrained or unwilling to give mouth-to-mouth, compressions alone, without stopping, can still save a life, because the chest compressions are the part that keeps blood moving.
What About Mouth-To-Nose Resuscitation?
The kiss of life is not always delivered to the mouth. Mouth-to-nose resuscitation uses the very same principle, your expired air with the same head-tilt and chin-lift, but the rescuer seals their lips around the victim's nose instead and keeps the victim's mouth closed so the breath travels down the airway. It is an accepted alternative rather than a separate technique.

When would you reach for it? It comes into its own whenever the mouth is hard to use, such as a serious facial or jaw injury, a mouth that will not open, or vomit that cannot be cleared. It is also a natural choice in the water. In a drowning rescue, a trained rescuer can begin in-water rescue breathing while still swimming the casualty to safety, sealing over the nose and delivering breaths at roughly 12 to 16 per minute for about a minute, because keeping the lungs supplied with oxygen buys precious time.
Drowning is also a useful reminder that breaths are not always optional extras. Standard cardiac arrest care leans heavily on compressions, but drowning is fundamentally a problem of lost oxygen, so current guidance recommends giving rescue breaths first in these cases, often five initial breaths before chest compressions. The same logic explains why rescue breaths still matter so much for children and infants, whose collapses are far more often caused by a breathing problem than a heart problem. (For the everyday version of this question, see our piece on whether to breathe through the nose or the mouth during exercise.)
References (click to expand)
- http://users.rowan.edu/~farrell/hohb/Respiration%20Module/Respiration%20Handout.pdf
- Peter Safar, (1960) Resuscitation in the Dental Office Journal of the American Dental Society of Anesthesiology - PubMed Central (PMC) - National Center for Biotechnology Information
- In brief: Giving mouth-to-mouth resuscitation. InformedHealth.org. NCBI Bookshelf.
- The composition of gas given by mouth-to-mouth ventilation during CPR. Chest. PubMed.
- How to perform CPR - on adults, children and babies. Healthdirect Australia.
- Drowning: Clinical Management. StatPearls. NCBI Bookshelf.