Table of Contents (click to expand)
- What’s The Difference Between Pain Threshold And Pain Tolerance?
- Dolorimetry And How We Measure Pain
- The Dol Pain Scale: What 1 Dol To 10.5 Dols Was Supposed To Feel Like
- How Do The Worst Pains Compare?
- The Brain’s Perception Of Pain Plays A Role In How Much Pain Someone Can Tolerate
- Do Men And Women Feel Pain Differently?
- Can You Pass Out Because Of Excessive Pain?
- Is There A Maximum Amount Of Pain A Human Can Feel Without Dying?
There is no single, universal limit to how much pain a human can handle. Tolerance varies enormously with genetics, past experience, psychological state, and even cultural beliefs. In the 1940s, Cornell researchers tried to quantify it with the "dol" scale (0 to 10.5 dols, with second-degree burns hitting about 8), but it was abandoned because the same stimulus produces wildly different reported pain across people. The most painful conditions documented in clinical research include cluster headaches (often rated 9.7/10), kidney stones, severe burns, and femur fractures. Extreme pain can trigger fainting (vasovagal syncope), but pain itself doesn't directly kill.
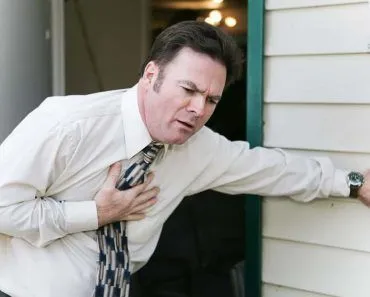
When you slam your finger in a car door, it probably feels like the worst possible pain in that instant, but a few minutes later, when the searing ache begins to dull, we return to reality.
We remember that we hadn’t just been hit by a bus, shot by an arrow, or dismembered by a horse and carriage. From that perspective, all seems right with the world.
Yet it makes one wonder…what is the worst possible pain for human beings? More importantly, how much pain can we actually handle before passing out, dying, or completely losing our minds?
What’s The Difference Between Pain Threshold And Pain Tolerance?
Pain threshold and pain tolerance sound interchangeable, but in pain research they are two distinct points on the same dial.
The pain threshold is the moment a sensation first registers as painful. If a clamp slowly tightens on your wrist, the exact pressure at which “tight” tips into “ouch” is your threshold. The International Association for the Study of Pain (IASP) defines it as the least experience of pain a person can recognize as painful, and it turns out to be surprisingly consistent across healthy adults.
Pain tolerance, on the other hand, is the upper end. It is the greatest level of pain you are willing to accept before you pull your hand away, ask for medication, or pass out. The IASP defines it as the maximum intensity of a pain-producing stimulus a person is willing to endure. Unlike threshold, tolerance varies enormously between people, because it depends on attention, emotion, expectation, and context as much as on the raw signal coming from the nerves.
A quick side-by-side:
| Concept | What it measures | Varies between people? |
|---|---|---|
| Pain threshold | The lowest stimulus intensity that first registers as painful. | Only a little. Most healthy adults sit in a fairly narrow band. |
| Pain tolerance | The maximum pain a person is willing to accept before stopping. | A lot. Genetics, mood, training, and culture all push the dial. |
So when someone says they have a “high pain tolerance,” they are not claiming they feel less pain at the start. They are claiming they can stay in the painful experience longer before tapping out. That distinction matters once you start comparing pain scales, because every scale (numeric, McGill, dol) is really measuring some mix of these two things.
Dolorimetry And How We Measure Pain
Both pain threshold and pain tolerance are arbitrary without some sort of scale to measure them on. How do we quantify that being punched is more painful than being pinched?
So, in their efforts to quantify pain, researchers Hardy, Wolff, and Goodell at Cornell University devised an experiment in which they exposed subjects' skin (blackened to minimize reflection) to focused heat from a lamp for three seconds at a time. They tested over 70 medical students and 13 women in labor, conducting hundreds of measurements, and asked subjects to report their pain levels.
Based on the Latin word dolor (pain), they created a unit of measurement for pain (the dol). One dol was the just noticeable difference between one pain intensity and another. Based on this, they created a 0 to 10.5 dol scale.
Many of the subjects reported feeling about 8 dol when they sustained second-degree burns. Beyond this point, pain became difficult to quantify. This method of measuring pain sensitivity is called dolorimetry.
This unit of measurement never really caught on in the scientific community. For starters, hardly anyone could reproduce their results. Second, pain is a subjective experience that depends on one’s emotional state at the time, their psychological outlook, as well as gender, age, and genetics.
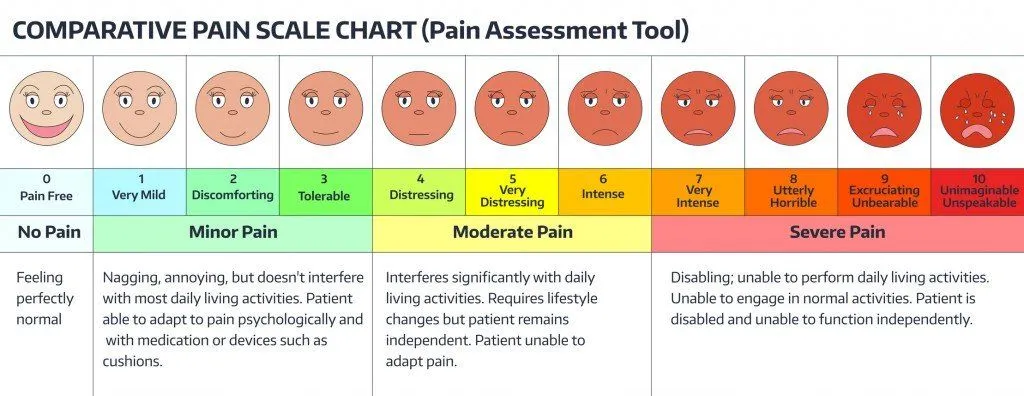
That’s the reason doctor’s offices still use those smiley-face charts (of which there are several types as well) when they ask you how much pain you’re experiencing. If you said, “Approximately 3.5 dols, the doctor probably wouldn’t even know what you meant, but when you point to an animated frowning face with tears in its eyes, the doctors understand.
As mentioned above, physical, psychological, and genetic factors all play a role in the subjective perception of pain for human beings, making precise quantification and comparison nearly impossible.
Scientists are making progress toward more objective pain measurement. Researchers using fMRI brain imaging combined with machine learning have shown promise in decoding pain intensity from brain activity patterns. A 2025 review highlighted advances in multimodal pain biomarkers that combine neuroimaging, molecular markers, and psychosocial data. While a universal, objective pain measurement tool remains elusive, these advances may eventually allow doctors to assess pain more precisely than smiley-face charts.
The Dol Pain Scale: What 1 Dol To 10.5 Dols Was Supposed To Feel Like
The dol scale didn’t survive contact with clinical reality, but it is worth seeing what Hardy, Wolff, and Goodell actually built, because the modern web is full of “how many dols is childbirth?” questions that the original paper never claimed to answer.
Here is the design. The three Cornell researchers shone a calibrated heat lamp on a small patch of blackened forehead for three seconds. Subjects reported when the heat first became painful (the threshold) and when it became unbearable (the ceiling). Between those two points, they could reliably tell apart 21 step changes in intensity. Each of those steps was called a just noticeable difference, or JND. They grouped JNDs in pairs and called every pair one dol. That gave them a scale running from 0 dols (no pain) to 10.5 dols (the ceiling, beyond which subjects could not discriminate further).
Roughly where common stimuli landed in the original experiments:
| Dols | What it corresponded to |
|---|---|
| 0 | No pain. |
| 1 to 2 | The first faint sting from the heat lamp, just above threshold. |
| 4 to 6 | Sustained, clearly unpleasant heat. |
| 8 | Approximately the intensity at which subjects sustained second-degree burns on the test patch. |
| 10.5 | The ceiling. Subjects could no longer tell stronger stimuli apart. |
The scale never extended past 10.5 dols. Modern claims that “kidney stones are 50 dols” or “childbirth is 57 dols” (the viral infographic version usually misspells the unit as “del,” as in “a human can bear 45 del and childbirth reaches 57 del”) are inventions; the original instrument had no way to measure pain beyond the ceiling, and the dol unit was tied to one very specific stimulus (radiant heat on a small skin patch). That is part of why the scale was quietly abandoned. The other reason is the one mentioned above: outside the original Cornell lab, almost no one could reproduce the same dol values on the same subjects. By the 1960s, clinicians had moved on to the numeric and verbal descriptor scales we still use today.
The dol is now a piece of pain-research history rather than a working unit, which is also why doctors today ask “Rate your pain 0 to 10” instead of handing you a dolorimeter.
How Do The Worst Pains Compare?
If the dol scale didn’t survive contact with reality, what do researchers actually use to compare pain across conditions? Mostly, three tools.
The Numeric Rating Scale (NRS, 0 to 10) is the clinical workhorse. It is what you are handed in an emergency room: “Rate your pain right now.” It is quick, repeatable, and useful for tracking the same patient over time, though the same “8 out of 10” means different things to different people.
The McGill Pain Questionnaire (MPQ), developed by Ronald Melzack at McGill University in 1971, goes deeper. Patients pick from lists of descriptors (throbbing, burning, stabbing, gnawing, exhausting), separating the sensory, affective, and evaluative dimensions of pain. In a 1984 study, Melzack used the MPQ to score labor pain and found it ranked among the most intense pains the questionnaire had ever recorded, with first-time mothers reporting more severe pain than mothers who had given birth before.
For insect stings specifically, entomologist Justin Schmidt built the Schmidt Sting Pain Index, a 1 to 4 scale most recently published across 96 species in a 2019 Toxins paper. Three insects tie at the top: the bullet ant, the tarantula hawk wasp, and the warrior wasp. Schmidt famously described the bullet ant’s sting as “pure, intense, brilliant pain, like walking over flaming charcoal with a three-inch nail embedded in your heel.”
Beyond these scales, cross-condition comparison gets genuinely fuzzy. There is no validated scientific ranking that says a kidney stone is exactly so many units worse than childbirth. The most researchers can do is line up patient-reported NRS averages from separate studies, which is why the cluster headache rating of 9.7 out of 10 carries weight: it comes from surveys of people who have actually lived with cluster headaches, not from a one-time lab experiment.
Putting numbers on a multi-condition ranking is genuinely hard, but here is roughly how the medical literature orders the conditions patients most often nominate as the worst pain of their lives. Where a study used a 0 to 10 scale, the figure in brackets is the mean rating from patients with that condition.
- Cluster headache (≈9.7/10). In the 2021 International Cluster Headache Questionnaire of 1,604 patients, the mean attack rating was 9.7 out of 10, and 72% rated their attacks at the absolute maximum of 10. The condition is sometimes called the “suicide headache” because of its association with elevated suicidal ideation.
- Trigeminal neuralgia. An electric-shock pain in the face, set off by something as small as a breeze or chewing. Often described in clinical literature as among the most severe pains in medicine, and tied to significantly higher rates of suicidal thoughts than the general population.
- Complex regional pain syndrome (CRPS). A persistent burning pain, usually in a single limb after an injury, that the McGill Pain Questionnaire frequently scores higher than active labor or amputation of a digit.
- Kidney stones. Most adults who have passed a stone describe it as the worst pain they have ever felt. The pain is colicky, wave-like, and concentrated in the flank or lower abdomen as the stone moves down the ureter.
- Severe burns. Third-degree burns are paradoxical in that the burned region itself can be numb (the pain nerves are destroyed), but the surrounding partial-thickness burns and the daily dressing changes that follow are routinely rated 9 or 10 out of 10 in burn-unit studies.
- Childbirth (unmedicated). In Ronald Melzack’s 1984 McGill study, first-time mothers giving birth without an epidural rated their pain on the McGill Pain Questionnaire higher than almost any other clinical population the instrument had been used on. Patients who have had both a kidney stone and a vaginal delivery are split roughly evenly on which was worse.
- Femur (thigh-bone) fracture. The femur is one of the strongest bones in the body, and breaking it tears through a heavily innervated muscle envelope. Patients arriving in the emergency department with isolated femur fractures consistently rate the pain 9 or 10 out of 10 before opioid analgesia.
- Bullet ant sting. The only non-clinical entry on this list, included because it tops Justin Schmidt’s 1 to 4 sting-pain index at the maximum 4.0. Schmidt described it as “pure, intense, brilliant pain, like walking over flaming charcoal with a three-inch nail embedded in your heel,” and the pain lasts up to 24 hours.
A few things worth noting about this ranking. First, the order is fuzzy beyond the top entry; cluster headache is unusually well documented because thousands of patients have rated it on the same scale, but most other comparisons rely on smaller studies with different instruments. Second, the list is biased toward acute pains that can be measured during a single episode. Chronic pain conditions like fibromyalgia or persistent back pain rarely score 10 out of 10 on a single rating, but they can be just as destructive over years.
The Brain’s Perception Of Pain Plays A Role In How Much Pain Someone Can Tolerate
As a child, imagine that you were protected from every possible danger by your parents (e.g., no climbing trees, no roughhousing, no bikes, no sports, etc.). If you have never experienced a sprained ankle, a blackened eye or a broken bone, your pain threshold might likely be low. Another child who grew up scraping their knees, spraining their ankles, and being in and out of casts would likely develop a higher tolerance for pain. Once you break a few fingers falling off your skateboard, a bruised elbow doesn’t really seem that bad, right?
This experience is backed by research and sometimes in odd ways. During World War II, Henry Beecher found that injured soldiers reported significantly less pain than civilians with comparable injuries. For the soldiers, their wounds meant they were leaving the battlefield alive. The injury was associated with relief, not distress, which dramatically reduced their pain perception.
Reasonably, sports persons and dancers are found to have a higher pain tolerance than, say, a writer who spends their entire day hunched in front of a computer.
More bizarrely, if your brain believes there is no pain, then you stop feeling pain. This is called the placebo effect, and it applies to more than just pain. It is the power of belief on how your body feels, which includes pain. So, the attitude of some cultures saying “mind over matter” have a point, even if in a roundabout way.
But, of course, the brain is complicated and we’re still unsure of just how the brain processes pain.
So, even though you and I might experience pain differently, it is likely that some times are still going to max anybody out.
Among the most painful experiences reported by patients are cluster headaches (often called "suicide headaches," rated 9.7 out of 10 in research studies), kidney stones, severe burns, and bone fractures, particularly the femur, the longest bone in the body. Childbirth is also consistently rated among the most painful experiences. The popular claim that testicular injury pain is "equivalent" to childbirth has no scientific basis, as pain experiences are too subjective to compare directly across different types of stimuli.
Heartbreak Hurts
Social pain is a real pain. We reflect this in the way we talk about such pain, “You hurt my feelings,” or “I’m heart broken.” The thought of losing a loved one is the same as actual pain for the brain. The thought or event activates two parts in the brain, namely the dorsal anterior cingulate cortex (dACC) and anterior insula (AI), that are also activated when you feel distressing physical pain. You might not be able to measure this on a dol or visual analog scale, but it is real!
Do Men And Women Feel Pain Differently?
If you have ever wondered whether women really do handle more pain than men, the honest answer from pain research is yes and no, and the difference depends on what you mean by “handle.”
Across hundreds of laboratory and clinical studies, women report higher pain intensity than men for the same standardized stimulus (a thermal probe, a pressure cuff, a small electric shock). They are also disproportionately represented in nearly every chronic pain condition: migraine, fibromyalgia, temporomandibular disorder, and irritable bowel syndrome are all roughly two to three times more common in women than in men. Jeffrey Mogil’s 2012 review in Nature Reviews Neuroscience documented these gaps in detail and concluded that the evidence for clinical and experimental sex differences in pain is overwhelming.
The picture flips, though, when you ask about tolerance for the most extreme pain. Unmedicated labor produces some of the highest McGill Pain Questionnaire scores ever recorded, and women routinely move through it and out the other side. The simplest reading is that women, on average, register pain at a slightly lower threshold and report it more honestly, but their tolerance for pain that has meaning attached (a baby, a marathon, a recovery) is not lower than men’s.
The biology behind the gap is genuinely mixed. Estrogen modulates several pain pathways and can amplify or dampen the signal depending on which receptor it lands on. Variants of the COMT and OPRM1 genes change pain sensitivity differently in men and women. And on top of all that sits a sociocultural layer: men in many cultures underreport pain because admitting to it is treated as weakness, which inflates the apparent difference in laboratory studies. Bartley and Fillingim’s 2013 review in the British Journal of Anaesthesia lays out the biological, psychological, and social inputs that pull these numbers in different directions.
The takeaway is not that one sex is “tougher” than the other. It is that pain is processed through a body and a brain that are themselves shaped by hormones, genes, and expectations, and those inputs differ on average between men and women. Asking who can take more pain is a bit like asking who is taller; the averages differ, but the spread within each group is wider than the gap between them.
Can You Pass Out Because Of Excessive Pain?
If you experience intense pain, your brain can push the emergency shut down button. Fainting because of intense, unbearable pain is called a vasovagal syncope.
Many people have experienced it and the reason behind this is the lack of blood supply to the brain. When you experience a sudden and sharp pain, it can overstimulate the vagus nerve, which is responsible for controlling your heart rate (HR) and blood pressure (BP). So the interruption in its working can lead to a drop in the HR and BP. This affects the blood supply to the brain which causes stress, which results in fainting. The amount of pain which could cause fainting depends on the person’s tolerance towards pain.
Just take our word for it…. and please don’t try to measure your own pain tolerance!
Is There A Maximum Amount Of Pain A Human Can Feel Without Dying?
It is one of the most-googled questions about pain, and the honest answer is that the ceiling is set by your brain, not by an objective threshold.
Pain itself is not a poison. It is a signal the brain constructs from incoming nerve activity, and the body has built-in shutoffs long before that signal can climb forever. Vasovagal syncope (covered above) is one of them: the system drops your blood pressure and you faint, which removes the conscious experience of pain.
Where pain genuinely raises the risk of death, the pathway is usually indirect. Trigeminal neuralgia, sometimes called the “suicide disease” in clinical literature, is associated with significantly elevated suicidal ideation. In a 2025 study in the Journal of Pain Research, 34.6% of patients reported some thoughts of suicide in the prior two weeks, with rates higher among those with the most severe pain. Cluster headache shows a similar pattern, which is why the condition has long been called a “suicide headache.”
The reverse case is instructive. People born with congenital insensitivity to pain with anhidrosis (CIPA) cannot feel pain at all, and the result is not freedom. According to MedlinePlus, they incur repeated severe injuries, including unintentional self-injury such as biting the tongue, lips, or fingers, which can lead to spontaneous amputation of the affected area. Pain, as miserable as it is at the top of the scale, is what keeps the rest of us from doing that.
So the practical answer to “how much pain can a human feel without dying?” is: the ceiling is whatever your brain allows you to stay conscious through, and that varies from person to person. There is no universal dol or NRS number that means “fatal.”
References (click to expand)
- Hardy, J. D., Wolff, H. G., & Goodell, H. (1940). Studies on Pain: A New Method for Measuring Pain Threshold and Observations on Spatial Summation of Pain. Journal of Clinical Investigation.
- Hardy, J. D., Wolff, H. G., & Goodell, H. (1947, November 1). Studies On Pain: Discrimination Of Differences In Intensity Of A Pain Stimulus As A Basis Of A Scale Of Pain Intensity. Journal of Clinical Investigation. American Society for Clinical Investigation.
- Laatikainen, L. M., Sharp, T., Harrison, P. J., & Tunbridge, E. M. (2013, April 16). Sexually Dimorphic Effects of Catechol-O-Methyltransferase (COMT) Inhibition on Dopamine Metabolism in Multiple Brain Regions. (T. Burne, Ed.), PLoS ONE. Public Library of Science (PLoS).
- Noble, B., Clark, D., Meldrum, M., et al. (2005). The Measurement of Pain, 1945–2000. Journal of Pain and Symptom Management.
- Weisenberg, M., Tepper, I., & Schwarzwald, J. (1995, November). Humor as a cognitive technique for increasing pain tolerance. Pain. Ovid Technologies (Wolters Kluwer Health).
- Tajet-Foxell, B., & Rose, F. D. (1995, March 1). Pain and pain tolerance in professional ballet dancers. British Journal of Sports Medicine. BMJ.
- Schmitz, A., Vierhaus, M., & Lohaus, A. (2012, June 19). Pain tolerance in children and adolescents: Sex differences and psychosocial influences on pain threshold and endurance. European Journal of Pain. Wiley.
- Eisenberger, N. I. (2012, May 3). The pain of social disconnection: examining the shared neural underpinnings of physical and social pain. Nature Reviews Neuroscience. Springer Science and Business Media LLC.
- Getting the measure of pain. Wellcome Collection.
- Cluster headache is one of the most intensely painful human conditions. PMC (2021).
- Innovations in acute and chronic pain biomarkers. PMC (2025).
- Melzack, R. (1984). A study of labour pain using the McGill Pain Questionnaire. Pain. PubMed.
- Schmidt, J. O. (2019). Pain and Lethality Induced by Insect Stings: An Exploratory and Correlational Study. Toxins. PMC.
- Suicidal Ideation and Self-Injury in Trigeminal Neuralgia. Journal of Pain Research (2025). PMC.
- Congenital insensitivity to pain with anhidrosis. MedlinePlus Genetics, NIH.
- Terminology. International Association for the Study of Pain (IASP).
- Pain Assessment. StatPearls. NCBI Bookshelf.
- Trigeminal Neuralgia. National Institute of Neurological Disorders and Stroke (NINDS).
- Complex Regional Pain Syndrome. NINDS.
- Kidney Stones. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
- Melzack, R. (1984). The myth of painless childbirth. Pain.
- Mogil, J. S. (2012). Sex differences in pain and pain inhibition. Nature Reviews Neuroscience.
- Bartley, E. J., & Fillingim, R. B. (2013). Sex differences in pain. British Journal of Anaesthesia.