When an organ is removed from the body, the empty space is filled in by encroaching organs around it. The small organ-shaped space would be edged into by the pancreas, stomach and liver. In the case of larger “gaps”, such as a removal of part of the intestine, bodily fluid would temporarily fill the space until connective tissue begins to form, ensuring that everything in your body’s cavities remain in the right place!
Hopefully, you will never have to worry about having one of your organs removed, but the fact is, sometimes it simply can’t be avoided. As we get older, things break down and may stop working, while in other cases, accidents, disease or trauma may cause irreparable damage.
There are a handful of organs that humans simply can’t live without, while there are others that can be removed without proving fatal. More specifically, human beings cannot live without your brain, heart, liver, kidneys and lungs, although a person can survive without only one lung or kidney (as we have two). When you imagine removing an organ, however, such as a spleen, a gallbladder, a kidney or part of the intestine, have you ever wondered what happens to that empty space?
What Happens To The Empty Space After An Organ Is Removed?
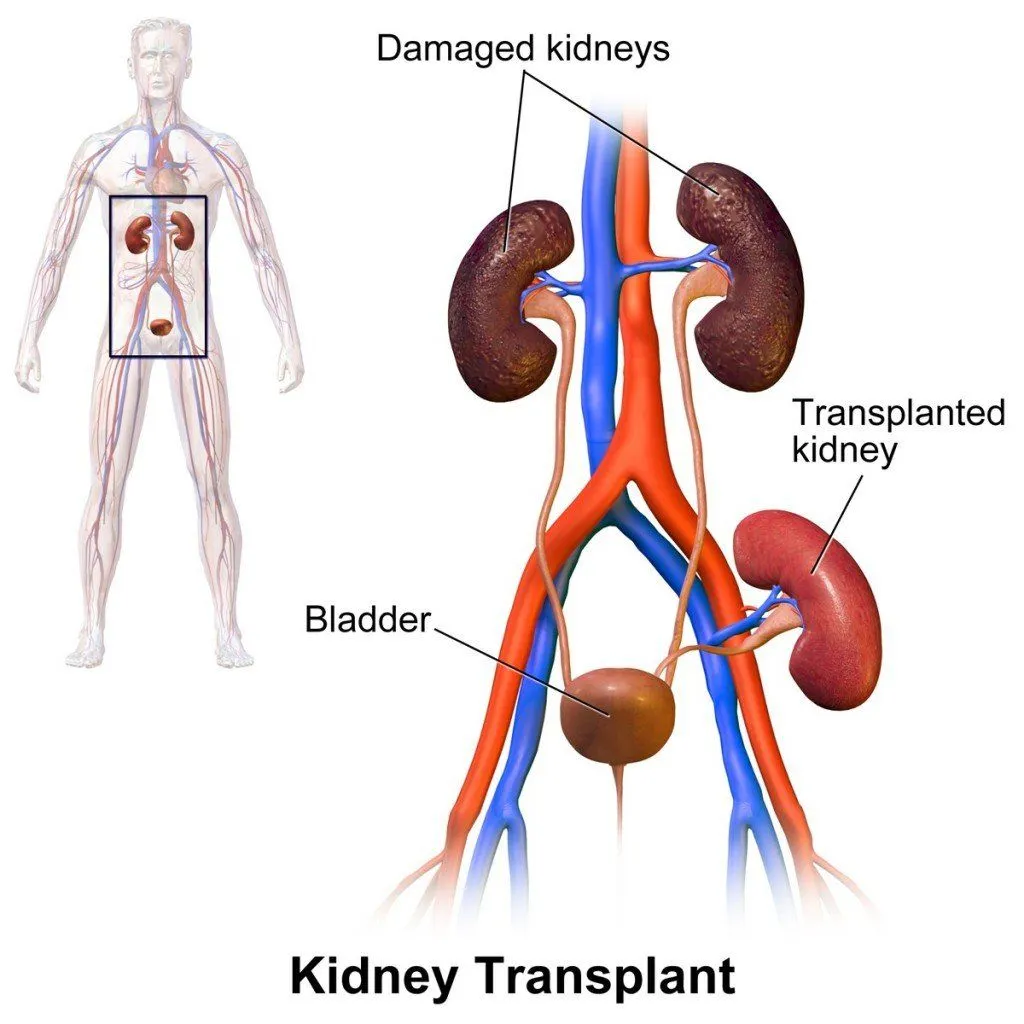
For those who don’t know, there are a number of organs that can be removed safely, which may leave a bit of empty space behind, including the spleen, stomach, gallbladder, colon, reproductive organs and appendix. You can also remove parts of the lungs, liver and intestines. Interestingly enough, kidney transplants are very common, but the non-functioning native kidneys usually aren’t removed; instead, the new kidney is placed in the lower abdomen (the iliac fossa, just above the groin) and connected to the iliac blood vessels and the bladder, a good distance lower than where the original kidneys sit.
Our bodies are divided into specific cavities, which do restrict the movement of our organs to some degree. For example, our heart isn’t going to slowly slip from the pericardial cavity, out of the thoracic cavity and land in the middle of the abdominal cavity. That being said, the layers of tissue dividing these cavities do have some amount of flexibility, as does the space within each individual cavity. Generally speaking, organs will remain in their designated area, although shifting and rearranging can happen. Imagine sucking in your stomach as far as you can, or filling your belly up with air; those simple muscle movements will cause compression and shifting of our organs, albeit a temporary change.
The body cavities are crowded places, and our organs simply fit in with one another as best they can. If you remove an organ, say the gallbladder, the empty space where that organ is would be filled in by encroaching organs around it. The small gallbladder-shaped space would be edged into by the pancreas, stomach and liver. In the case of larger “gaps”, such as a removal of part of the intestine, bodily fluid would temporarily fill the space until connective tissue begins to form, ensuring that everything in your body’s cavities remain in the right place!
Human bodies are remarkably adept at finding homeostasis in terms of pressure and comfort for our organs. Imagine standing in a crowded elevator with 10 other people. When 1 of those people depart at the next floor, the remaining people will subtly fill in that new gap, easing the pressure on the rest of the riders. The same thing is true in your body; your organs will naturally spread out, within reason, until there’s no empty space left.
The same principle holds for procedures like hysterectomy. After the uterus is removed, the small bowel and bladder gradually settle into the lower pelvis to occupy the space, while the surrounding ligaments and connective tissue keep neighboring organs anchored. Likewise, after a kidney is removed (a nephrectomy), the intestines and a small amount of fat shift over to fill the renal fossa, and the remaining kidney typically grows slightly to compensate.
How Do Your Organs Stay In Place (And Is There Any Empty Space In There)?
If our organs are simply packed together, what stops them from sliding around like loose groceries in a shopping bag? The answer is a remarkable internal scaffolding centered on a thin, slippery membrane called the peritoneum. This serous membrane lines the walls of the abdominal cavity and also drapes over the organs themselves, forming two layers (a parietal layer against the body wall and a visceral layer hugging the organs) with a narrow gap between them known as the peritoneal cavity.

So is there a big pocket of empty space inside you? Not really. The peritoneal cavity is what anatomists call a potential space, normally holding only about 50 to 100 millilitres (roughly 1.5 to 3.5 fl oz) of serous fluid. That tiny film of lubricant is what lets your organs glide smoothly past one another as you breathe, eat and move, rather than grinding together.
The actual holding-in-place job falls to two structures that are simply folds of the peritoneum. The mesentery is a double-layered fan of tissue that suspends the small and large intestine from the back wall of the abdomen, carrying their blood vessels, nerves and lymphatics along for the ride. Peritoneal ligaments tether other organs to the abdominal wall or to each other. Organs slung inside the cavity (intraperitoneal) can shift a little, while those pinned against the back wall (retroperitoneal), such as the kidneys, stay largely fixed. So your insides are not floating in a void; they are crowded, anchored and lubricated, which is exactly why a removed organ leaves so little usable "space" behind.
Do Your Organs Rearrange Themselves After Surgery?
A popular idea floating around is that you can take organs out, put the rest back in roughly any order, and the body will magically sort itself out. That is a myth worth puncturing. Organs do not autonomously navigate back to their "correct" addresses. During an operation the surgical team physically moves and then repositions the organs they handle, and the anchoring tissue we just met, the mesentery and ligaments, keeps everything broadly where it belongs once the abdomen is closed.
What actually changes the internal landscape after surgery is scar tissue. Bands of fibrous tissue called abdominal adhesions form as part of healing, and they can make loops of bowel or other organs stick to one another or to the abdominal wall. According to the U.S. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), adhesions develop in more than 9 out of every 10 people who have open abdominal surgery. Keyhole (laparoscopic) surgery, which uses small incisions, tends to produce fewer of them.
The good news is that most people with adhesions never notice them. When they do cause trouble, it is usually because the bands kink, twist or compress the intestine rather than because an organ has wandered off. The most serious complication is a bowel obstruction, where the gut becomes blocked, which is a medical emergency that can show up days after the operation or, occasionally, many years later. So the honest answer to "do organs rearrange themselves?" is no: they are placed back deliberately, held by their connective tissue, and the only real reshuffling comes from scar tissue, not from organs steering themselves home.
For people who choose to donate all their organs after death, there has been a new development, in an effort to maintain the integrity of the body for viewing and ceremonial circumstances. To keep the body’s internal cavities somewhat stable (volumetrically speaking), there have been some advancements in organ replacements. With the advent of 3D-printing technology, a number of researchers and pioneers have begun 3D printing the organs that are being removed, and then filling that empty space with replicas.
 After a person has died, this approach is the only way to “fill the space” of missing organs, but for living donors, your healthy organs will gladly take the opportunity to stretch out and fill every spare centimeter!
After a person has died, this approach is the only way to “fill the space” of missing organs, but for living donors, your healthy organs will gladly take the opportunity to stretch out and fill every spare centimeter!
References (click to expand)
- Sun, D.-P., Lee, L.-H., Tian, Y.-F., Zheng, H.-X., Kuo, J.-R., & Wang, C.-C. (2018, July). How to Deal with the Empty Space After Organ Removal for Transplantation: A Single Medical Center Experience. World Neurosurgery. Elsevier BV.
- Chest Organs Anatomy, Diagram & Function | Body Maps. Healthline Media, Inc.
- Unit 2: Anatomy and Physiology of Organ Systems - www.austincc.edu:80
- Abdominal Adhesions. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), NIH.
- Anatomy, Abdomen and Pelvis: Peritoneum. StatPearls. NCBI Bookshelf.
- Peritoneum: Anatomy, Function, Location & Definition. Cleveland Clinic.
- Rojas-Canales, D. M., Li, J. Y., Makuei, L., & Gleadle, J. M. (2019). Compensatory renal hypertrophy following nephrectomy: When and how? Nephrology (Carlton).