It depends on the kind of unconsciousness. Under general anesthesia, fainting, or brain death, the cortex isn't processing signals at all, so no pain is consciously felt. In coma and especially the minimally conscious state, brain imaging suggests pain perception is at least partly preserved, even if the patient can't tell you so.
One reason why pain is difficult to study is that our subjective experience of pain (how it “feels” to feel pain) and physical manifestations of pain (having pain receptors and the brain’s recognition of pain) are different. After all, animals have pain receptors, but we don’t know if they “feel” pain the same way we do.
Interestingly, consciousness (and self-awareness) was considered an important criterion for an organism to “feel” pain, which is why psychologists thought babies couldn’t feel any pain for a very long time. Imagine that!
Given that, usually, we can only tell if someone is in pain and to what degree if we ask them, but what about when we’re unconscious?
What Does Science Say?
One way to investigate this idea is to ask caregivers or attenders who frequently deal with unconscious people. When medical doctors were asked, in a 2009 study, whether people in a vegetative or unconscious state could experience pain, 56% of them said yes, and 68% of paramedical caregivers also concurred.
We can’t solely rely on their word though. It has been historically unwise to conclude from subjective second-hand experiences, even if they come from people we consider experts on the issue. After all, one’s mind can be deceptive. It’s possible to mistake any response as a response to pain. To avoid falling into the same trap, we must start by looking at the physiology of the brain and go from there.
How Pain Works In The Brain
The brain is a complex organ, so not every process in the brain can be accounted for; the amount of information is simply too much to handle. To make things more manageable, psychologists tend to record which parts of the brain respond to particular stimuli and try to assign certain functions to the activated parts based on the stimulus administered. These tend to be generalizations, but they get the job done!
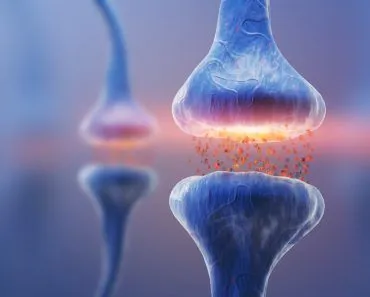
Applying the same methodology, scientists qualitatively split the experience of pain by the brain into three parts: the “cognitive-evaluative”, the “motivational-affective”, and the “sensory-discriminative”, which in simpler terms means the emotional response we have to pain, how pain affects our motivation, and the brain’s sensory experience of pain, respectively. What we’re interested in is the brain’s experience of pain, and how it perceives it.

The pain-related part of the brain is mostly controlled by parts of the thalamus, the frontal cortex and the connections between them (along with other parts of the brain). Schnakers’ team also found a difference in how the sensory-discriminative part of the brain responded to pain in patients in the vegetative state vs. those who were minimally conscious. In patients in the vegetative state, the cortex appeared to react strongly to pain, running many cortical processes, but there was a disconnection observed in the neural pathways between the thalamus and cortex and within the cortex. In minimally conscious patients, however, such a disconnect was not found. Additionally, there was a clear activation of the anterior cingulate, connected to pain experience, which wasn’t found in patients in the vegetative state.
What About Anesthesia, Coma, Sleep, And Brain Death?
Vegetative-state research is the cleanest experimental window on this question, but it isn't the kind of unconsciousness most people are asking about. Here's how the evidence stacks up in the more familiar scenarios:
General anesthesia. Properly delivered anesthetics like propofol don't just put you to sleep; they break the long-range communication in the cortex that's needed to actually perceive pain. Noxious signals still reach the brain, but they aren't integrated into conscious experience. The rare exception is accidental awareness during general anesthesia; the UK's large NAP5 audit (Pandit et al., 2014) put its incidence at roughly 1 in 19,000 cases, rising to about 1 in 8,000 when neuromuscular blockers are used. Roughly half of those cases involved distress or pain.
Fainting (vasovagal syncope). Fainting is a brief drop in blood flow to the brain that lasts only seconds. Without enough cortical perfusion, there's no conscious experience to register pain, which is why people typically don't feel hitting the floor; they only feel the bruise later.
Coma. A coma is unarousable unresponsiveness without sleep–wake cycles. By definition, comatose patients don't consciously perceive pain, but the nociceptive pathways are often intact, and clinicians cannot rule out residual processing in any given patient. That's why bedside tools like the Nociception Coma Scale-Revised are now used to spot behavioural signs of pain and guide analgesia. The International Association for the Study of Pain (IASP) is explicit that an inability to communicate is not evidence of an absence of pain.
Brain death. Brain death means an irreversible loss of all brain function, including the brainstem. With no cortex left to do the processing, brain-dead patients cannot feel pain. Any movements seen during organ retrieval are spinal reflexes, not signs of awareness.
Sleep. Sleep is a special case because it isn't full unconsciousness. The cortex still processes painful inputs in every sleep stage; whether they wake you up depends on how deep you are. Arousal thresholds are lowest in light NREM (stage 2) and highest in slow-wave and REM sleep, which is why a pinch can pull you out of a nap but barely register during deep sleep.
So What Does Being Unconscious Actually Feel Like?
People often ask the flip side of the pain question: forget whether it hurts, what does being knocked out actually feel like? The honest, slightly unsatisfying answer is that true unconsciousness doesn’t feel like anything. Researchers define it precisely as the inability to achieve any subjective experience: no sights, no thoughts, no sense of time ticking past. There is nothing it is “like” to be in that state, which is exactly why it is so hard to put into words afterwards.

The strangest part is the missing time. Under full general anesthesia, the brain is held in a single steady state for the length of the operation, so hours can collapse into what feels like a couple of seconds. Most patients remember nothing at all between the drug going in and waking up in the recovery room, and many are startled to learn the surgery is already over. That blank is also why coming round from anesthesia is not the same sensation as waking from a good night’s sleep.
This is where unconsciousness genuinely parts ways with ordinary sleep. When you sleep, your brain cycles through distinct stages all night, and a loud noise or a gentle nudge can pull you straight out of it. Clinical anesthesia holds that cycling still and shrugs off the same stimuli, which is part of what makes the time gap feel so seamless.
There is a twist, though. Being unresponsive is not always the same as having no experience at all. Anesthetists describe a state called disconnected consciousness, in which the mind generates its own content, usually dreams, while staying sealed off from the outside world. Dreaming turns out to be surprisingly common: around 27% of patients given propofol and 28% given desflurane report dreaming, even though none of them recall anything about the surgery itself. So being “out cold” can occasionally mean “quietly dreaming” rather than experiencing a total void.
Conclusion
Given the data, it’s likely that unconscious individuals (specifically, people in the minimally conscious state) do experience pain. However, there still isn’t enough research being done on pain, at least, not enough to comfortably compare degrees of pain or even detect it in some cases.
The study of the mechanism and experience of pain has wide-reaching consequences on how patients ought to be treated. If accurate estimates of the pain felt by unconscious patients aren’t made, doctors could risk over-administering or under-administering pain medication, both of which are problematic. Giving too little medication risks hurting the patient, whereas giving too much runs the risk of excessively sedating the patient and missing signs of returned cognition.
A lot is riding on such research. Sam Harris, a popular psychologist, in his book “The Moral Landscape”, argues that secular moral objectivity can be achieved once we can detect and quantify pain (and pleasure) properly. The burden of all secular ethics, therefore, rests on the shoulders of Science!

References (click to expand)
- Anand, K. J. S., & Hickey, P. R. (1987, November 19). Pain and Its Effects in the Human Neonate and Fetus. New England Journal of Medicine. Massachusetts Medical Society.
- Pandit, J. J. et al. (2014). 5th National Audit Project (NAP5) on accidental awareness during general anaesthesia. British Journal of Anaesthesia.
- IASP Terminology: Definition of Pain (inability to communicate does not negate experience of pain). International Association for the Study of Pain.
- Boly, M., Faymonville, M.-E., Schnakers, C., Peigneux, P., Lambermont, B., Phillips, C., … Laureys, S. (2008, November). Perception of pain in the minimally conscious state with PET activation: an observational study. The Lancet Neurology. Elsevier BV.
- Borsook, D., & Becerra, L. R. (2006, January 1). Breaking down the Barriers: fMRI Applications in Pain, Analgesia and Analgesics. Molecular Pain. SAGE Publications.
- Demertzi, A., Schnakers, C., Ledoux, D., Chatelle, C., Bruno, M.-A., Vanhaudenhuyse, A., … Laureys, S. (2009). Different beliefs about pain perception in the vegetative and minimally conscious states: a European survey of medical and paramedical professionals. Progress in Brain Research. Elsevier.
- Schnakers, C., Chatelle, C., Majerus, S., Gosseries, O., De Val, M., & Laureys, S. (2010, November). Assessment and detection of pain in noncommunicative severely brain-injured patients. Expert Review of Neurotherapeutics. Informa UK Limited.
- General Anesthesia: A Probe to Explore Consciousness. Frontiers in Systems Neuroscience. NCBI/PMC.
- Unresponsiveness ≠ Unconsciousness. Anesthesiology. NCBI/PMC.
- What’s the Difference Between Sleep and Anesthesia? BrainFacts.org, Society for Neuroscience.