Table of Contents (click to expand)
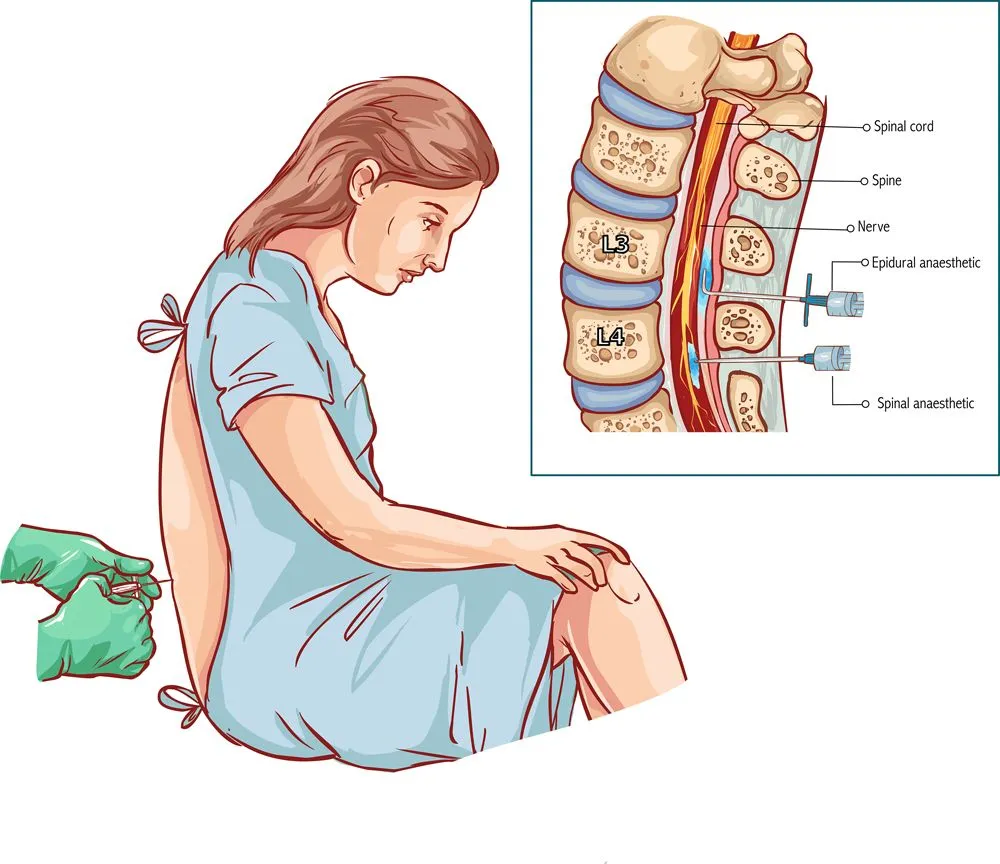
An epidural is a nerve block placed in the epidural space of the lower back, usually around L3–L4, during labor or surgery. A thin catheter delivers a low-dose mix of local anesthetic (typically bupivacaine) and an opioid (typically fentanyl), blocking pain at the spinal nerve roots while preserving touch and most muscle control. Roughly 75% of US vaginal births use one.
If you have personally given birth to a child, been in the room during a birth, heard about the experience from someone else, or simply watched the depiction of childbirth in movies or TV shows, you know that it is a uniquely beautiful and potentially excruciating act. The images of a mother’s face drenched in sweat, being told to “push” through the pain of labor, as she squeezes her partner’s hand into a pulp, are things that most of us have seen before.

However, modern medicine has progressed to the point where much of the pain of childbirth can be mitigated or blocked through various strategies, medications and minor procedures, including the use of an epidural. Before you decide whether to use an epidural during labor, or if you’re simply curious about this aspect of childbirth, the information below should clear up any uncertainty!
What Is An Epidural?
An epidural is a pain-relieving shot that many women receive during labor, and it effectively works as a nerve block. It is called an epidural because the medication is injected into the epidural space, the fat-filled gap that sits just outside the dura, the tough membrane that wraps the spinal cord and its fluid. In labor, the anesthesiologist threads the needle in at the lower back, usually between the L3 and L4 vertebrae (well below where the spinal cord itself ends), so the drug bathes the spinal nerve roots without touching the cord. Those nerve roots are the wires carrying pain signals from the uterus and birth canal up to the brain, and once they are numbed, the brain simply never gets the message. The same procedure is also used outside of pregnancy, in many surgeries (spinal and otherwise) and in the management of chronic pain. Unlike a general anesthetic, an epidural still allows for muscle function and for sensitivity to pressure and touch, often enough that women can shift position in bed (and, with a low-dose mix, sometimes stand and walk), while blocking the majority of the pain.
Epidurals come in a number of forms, including local epidurals, narcotic epidurals, local/narcotic mix, patient-controlled epidurals, continuous epidurals and intermittent epidurals. We will go into greater detail about these varieties below so the differences can be made clear.
Epidurals can be administered as a single injection, but this is often insufficient. For this reason, a catheter is usually attached to the injection site on the back, so additional medication can be easily delivered during the sometimes lengthy labor process.
Local Epidural
This is the standard or classic epidural, and it uses local anesthetics (such as bupivacaine, ropivacaine, or lidocaine) on their own to provide powerful pain relief. It is injected into the epidural space in the lumbar back (typically between L3 and L4), not into the cerebrospinal fluid itself (that would be a spinal block, a separate single-shot technique). A traditional, higher-concentration dose will numb you from the waist down, takes roughly 10–20 minutes to take full effect, and is then topped up through a catheter so the relief lasts as long as labor does. The trade-off is that a dense block can dull a woman’s ability to feel and push the baby out, so the second stage of labor may take longer. Other side effects include the inability to walk during labor, lowered blood pressure, and a small increase in the likelihood of an instrumental delivery (forceps or vacuum). Current evidence does not support the older worry that an epidural raises the risk of a Caesarean.
Narcotic Epidural
A narcotic-only epidural relies on opioid pain relievers, such as fentanyl, sufentanil, or morphine, to dampen the pain rather than producing a full nerve block. Because the local anesthetic component is removed, motor function is preserved almost entirely. It is sometimes used early in labor or in patients who cannot tolerate a drop in blood pressure from local anesthetic. Depending on the choice of opioid and the concentration, the pain relief can last anywhere from a few hours to a full day. The trade-off is that some opioid crosses the placenta, so babies may be a little sedated at birth and slightly slower to feed for the first day or two while their bodies clear the drug.
Local/Narcotic Mix
This is the workhorse of modern obstetric anesthesia and the form most American women actually receive. It blends a low concentration of local anesthetic with a small dose of opioid, most commonly bupivacaine at around 0.0625–0.1% combined with fentanyl at about 2 micrograms per millilitre. The local anesthetic takes the edge off the sharp pain at the nerve roots, while the opioid layers on additional relief without piling on more numbness. The lower concentration means mothers keep enough leg strength to shift position and push effectively, and the lower opioid dose minimizes the chance of a sleepy baby. When this mix is dialed low enough to preserve leg strength, it is often what hospitals advertise as a “walking epidural,” though in practice most labor units keep mothers in bed even when the block is light. It is generally considered the best-balanced strategy of the three.
Patient-Controlled, Continuous And Intermittent
In some cases, patient-controlled epidurals are called for, in which the release of narcotic medication through an IV into the catheter is determined by the patient. If you are experiencing a long labor, this might be an option. Also, there is a lock-out setting on the handheld release trigger to ensure that you don’t overmedicate yourself.
Intermittent epidurals can be “topped up” throughout the course of your labor if you have had a catheter injected and secured to your back. When the pain begins to return, the nurse or attending physician can easily administer more of the medication with a lag time of only a few minutes.
Continuous epidurals include the use of an IV bag and continuous, low-dose delivery of medication into the catheter. This is often preferred, because it reduces the swells of pain and relief that intermittent epidurals can cause.
Epidural Side Effects
There is a great deal of debate over the use of epidurals due to their potential side effects, some of which were explained above. While the idea of “sedating” your newborn baby or being unable to move during labor sound quite worrying, there are a number of other side effects to consider before deciding to use an epidural during labor.
The use of opioids in any context can result in certain side effects, such as topical itching of the skin and nausea or vomiting. The sedative nature of these drugs can also cause a drop in blood pressure, as well as fever or general soreness after the birth is over. Again, due to the numbness, some women have trouble urinating, or may become incontinent, as they are unable to tell when their bladder is full.
The rarer but more serious complications include nerve damage, infection, severe (“post-dural puncture”) headaches from an accidental dural tear, and respiratory issues if the block creeps too high. These are genuinely uncommon: the American Society of Regional Anesthesia and Pain Medicine puts the risk of lasting nerve damage from a neuraxial block at somewhere between 1 in 4,000 and 1 in 200,000 procedures, and when it does happen, the deficit is usually temporary. As mentioned above, a traditional dense local epidural can also lengthen the second stage of childbirth once the cervix is fully dilated.
Epidural Controversy
The advancement in epidurals over recent decades is remarkable, and when used properly and responsibly, they are widely considered safe and effective pain-management tools. The CDC’s National Center for Health Statistics reported that 75.4% of mothers having a singleton vaginal birth in the United States in 2024 used epidural or spinal anesthesia, up from 69.8% in 2016. Still, plenty of other approaches to pain management exist that do not involve narcotics or anesthetics. Human beings have been giving birth for tens of thousands of years without the help of such medicine, and many holistic practitioners and believers in natural medicine are staunchly against the use of drugs during childbirth.
While there are some risks to the use of an epidural, there is also something to be said for relieving pain when possible, particularly during a process often described as the most painful event a human can endure. Some people argue that deep breathing practices, support from a doula or birth partner, water immersion births, acupuncture, meditation and many other drug-free strategies will provide a more natural birth experience. There are positive and negative points on both sides, so ultimately, the decision to use or refuse an epidural is entirely personal. Be sure to discuss your decision with your doctor, along with your preferences and concerns, well before you go into labor!
A Final Word
Childbirth is a miraculous and momentous event in a woman’s life, but as the word “labor” implies, it takes a lot of work and perseverance through incredible pain. Epidurals, in various forms, can provide relief from the most severe discomfort of this magical moment, while also protecting the health and wellness of both mother and child.
References (click to expand)
- Birth: Learn More – Epidurals and other medications to ....
- Epidural – Everything You Should Know About It.
- Labor, S., & Maguire, S. (2008, December). The Pain of Labour. Reviews in Pain. SAGE Publications.
- Dozier, A. M., Howard, C. R., Brownell, E. A., Wissler, R. N., Glantz, J. C., Ternullo, S. R., … Lawrence, R. A. (2012, June 13). Labor Epidural Anesthesia, Obstetric Factors and Breastfeeding Cessation. Maternal and Child Health Journal. Springer Science and Business Media LLC.